Read more: A detailed case study on COVID-19 vaccine cold supply chain.

One of the most important strategies to win the fight against the pandemic involves the rollout of a vaccine at various vaccination sites. The goal is to vaccinate a critical mass of people within the shortest possible time to break the chain of virus transmission.
Indonesia has been among the most affected countries in terms of COVID-19 cases. As one of the world’s most popular tourism destinations, Bali has become one of the hardest-hit provinces in Indonesia and thus one of the priorities in the country’s vaccination program.
Bali province consists of nine regencies. The population profile, together with the land size and the number of available hospitals and community health clinics, is known to vary considerably in each of the regencies. That is why people have unequal access to vaccination services.
One way to overcome the challenges for such regions is through vaccination outreach. Under this strategy, several outreach sites, known as mobile clinics, are set up at various locations near the target populations.
The healthcare workers bring the vaccines from storage locations, such as hospitals, and commute to the outreach sites to administer them on a regular basis.
Buleleng is located in the northern part of Bali Island. While it is the largest regency in Bali province with 148 villages, it has the fewest number of hospitals and health centers. Moreover, they are not evenly spread out among the villages.
In this case study, we’re going to focus on the vaccine outreach for this particular regency and then the entire Bali province.

Bali province and its nine regencies
The vaccination outreach strategy has shown good results in the past. For example, a study by World Health Organization reported an increase in the vaccination rate from 25% to 57% in one region in Kenya with low population density and an increase from 54% to 82% in a high population density area.
In this case study, we’re first going to design a vaccination network to find the required number and location of outreach sites. The goal here is to maximize the vaccination coverage to include people that live nearby within a certain range.
Then, we’re going to design a vaccine supply network between health centers and the sites to determine the amount of vaccine doses that the sites need to keep. We’re also going to determine the required number of medical personnel and supply kits including syringes, needles, and alcohol swabs.
Transport routing is an important factor that needs to be considered in the development of an effective outreach program, especially when multiple outreach sites are involved. In such a scenario, the vaccination team will need to visit multiple sites to render the services at each site before returning to the base point, which can be the hospital or the health center where the vaccines are kept.
Greenfield Analysis (GFA)—also known as a center of gravity analysis—is a technique commonly used at the early stages of supply chain design to find the optimal number and locations of production facilities and/or distribution centers. The goal of GFA is to meet customer demand in the most cost-effective way.
In this case study, for GFA, fixed health centers are represented as production plants, outreach facilities as distribution centers, and maximizing vaccination coverage is equivalent to meeting customer demand.
The researchers built a GFA vaccine outreach model in anyLogistix supply chain design software and set the following inputs:
First, the researchers built a baseline model of the Buleleng vaccination network. In it, the existing 13 health centers served as vaccination sites. The villagers living nearby will have to travel to these centers to get vaccinated.
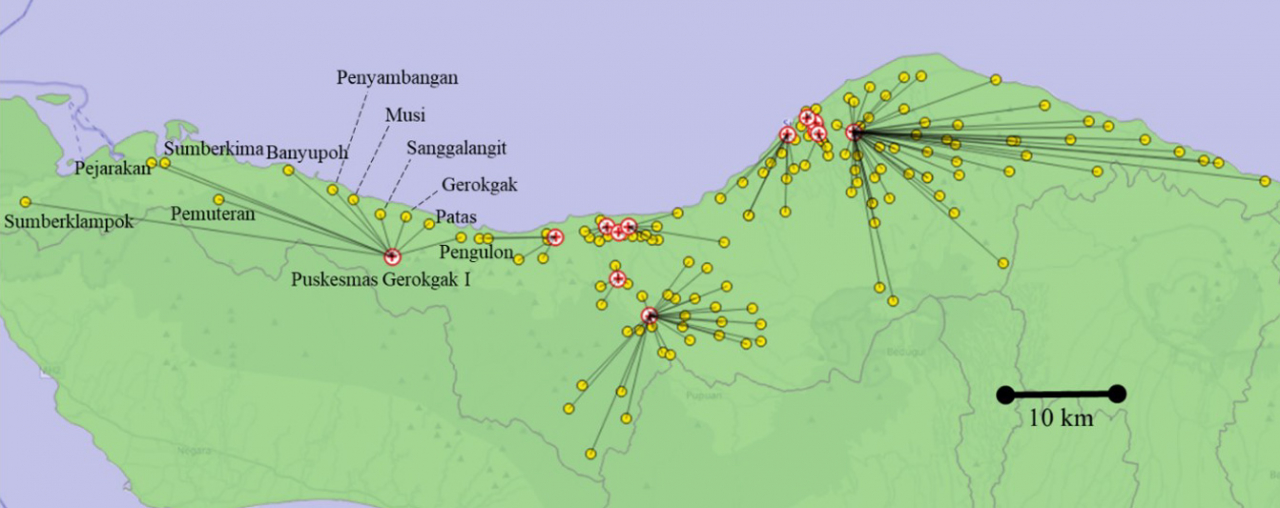
Vaccination network in the Buleleng baseline scenario. The red circles are health centers, and the yellow are the villages (click to enlarge)
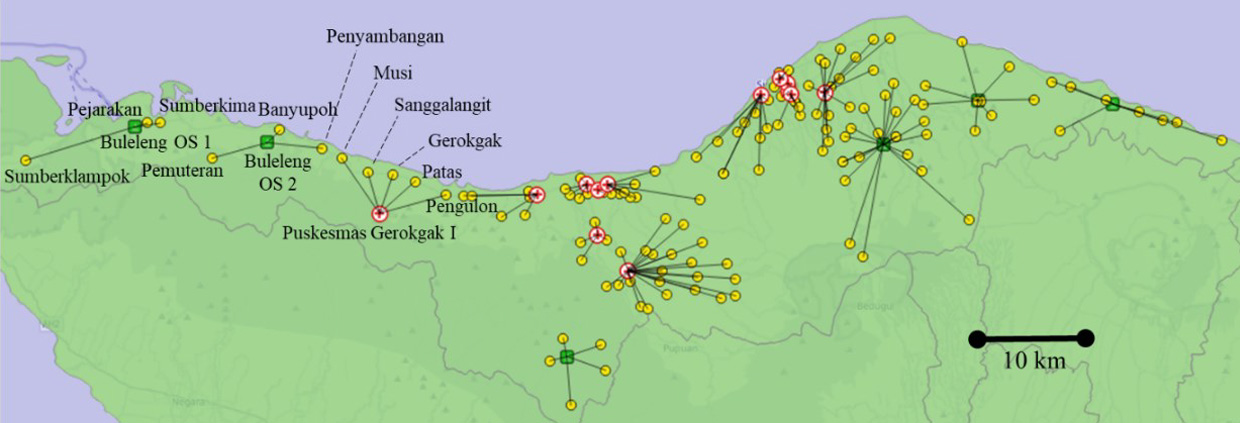
Vaccination network in the Buleleng outreach scenario (10-km range). The red circles are health centers, yellow are the villages, and green are new mobile clinics (click to enlarge)
In this scenario, every village must be located within 10 km and 3 km from a health center or an outreach site respectively. Within a 10-km range, six outreach sites are added to the pool of 13 health centers to serve the population of Buleleng.
In the baseline scenario, 5 out of 11 villages have a traveling distance of more than 10 km. But after performing GFA, all of these 11 villages are located within 10 km from the health center or outreach site.
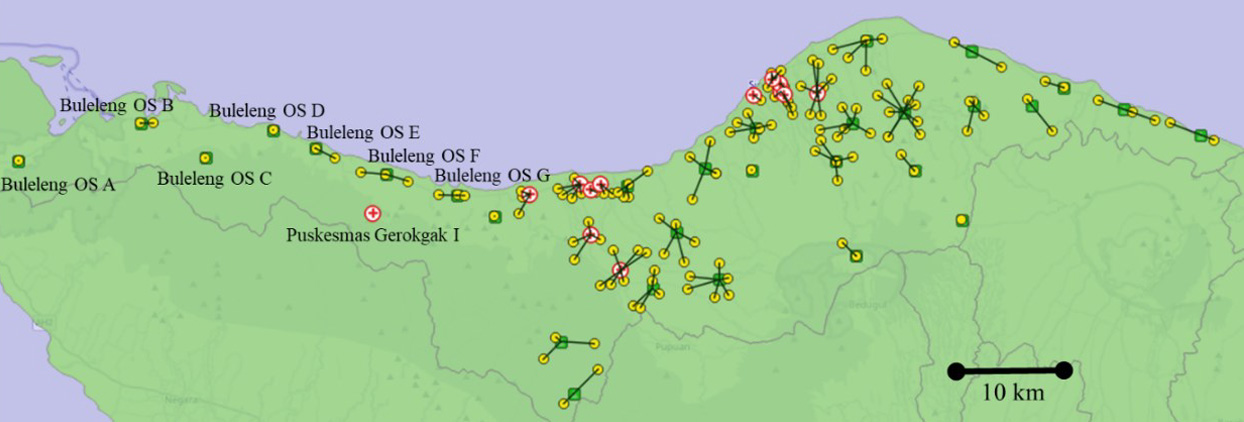
Vaccination network in the Buleleng outreach scenario (3-km range). The red circles are health centers, yellow are the villages, and green are new mobile clinics (click to enlarge)
The vaccination network within a 3-km range identified 30 outreach sites. In this scenario, only 12 health centers are used for vaccination instead of all 13. Six of the 11 villages, originally served by the same health center in the baseline scenario, are used as outreach site locations. So, the travel distance from villages to these new outreach sites become zero.
The average straight-line distance per person decreases significantly from 6.8 km (baseline) to 3.4 km (10-km range) and 1.1 km (3-km range).
Using Greenfield Analysis in anyLogistix, the researchers modeled the second step of the vaccine outreach planning—distribution network. They tested different network configurations for vaccine supply distribution from health centers to outreach sites for 3 and 10-km max distance.
They also identified that the total number of vaccinators required is 104 (10-km range) and 118 (3-km range). The highest 14-day stock amount required for any health center is 17,682 sets and 17,780 sets respectively.
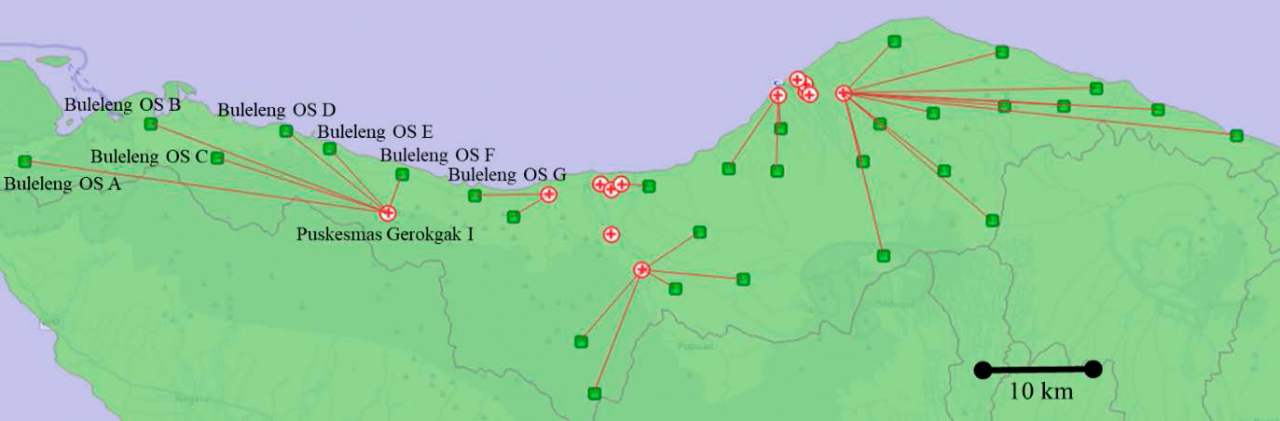
Vaccine distribution network in the Buleleng outreach scenario (3-km range). The red circles are health centers and the green squares are new mobile clinics (click to enlarge)
The researchers used the same 2-step Greenfield Analysis for the whole province with eight other regencies. They set an important rule: no village can be served by a health center or an outreach site outside of its regency. The rule was applied even when the distance from the other health center or outreach site to the village in the neighboring regency was shorter.
One of the findings was that regions with similar population numbers but different geographical characteristics could require a different number of outreach sites.
For example, Buleleng and Denpasar are the two largest regencies in terms of population size and so they have similar vaccine demands. However, the Buleleng population is spread out across 148 villages—the highest number of villages in Bali province. Meanwhile, Denpasar, the capital of Bali, is a city with 43 sub-districts, which are equivalent to villages on the administrative level.
As a result, the latter has the fewest number of villages among the nine regencies. So, the ratio of the number of health centers to the number of populations for Buleleng is much lower than that of Denpasar.
Overall, the researchers had to consider the regencies’ unique characteristics to get accurate results from the GFA model.
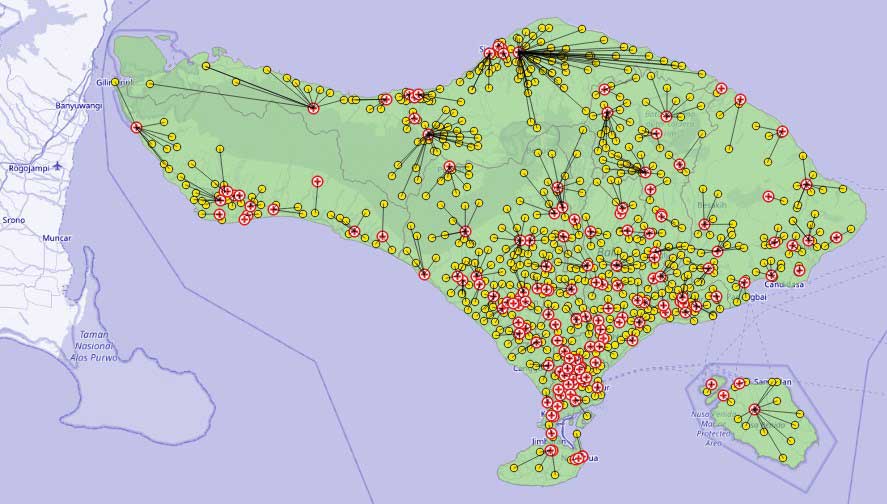
Bali vaccination network: baseline scenario without mobile clinics
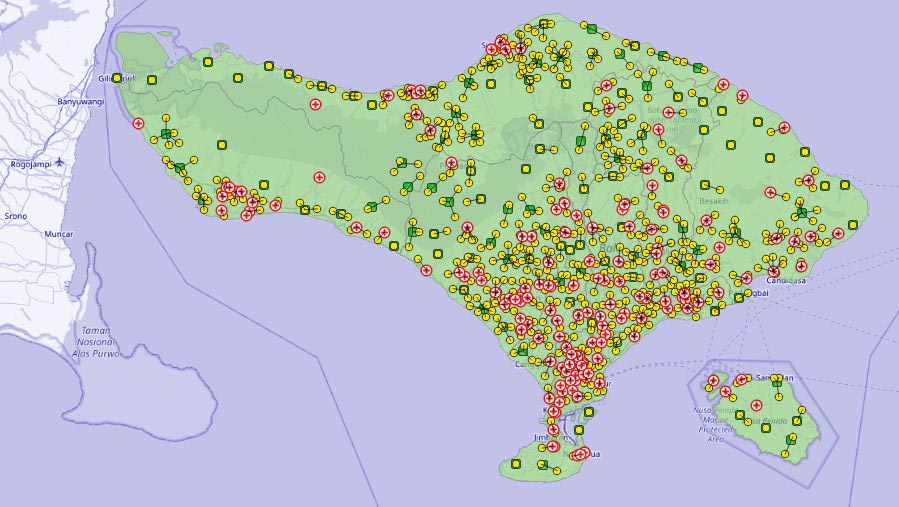
Bali vaccine outreach scenario (3-km range)
As a result, servicing 715 villages for the whole Bali province would require a total of 143 health centers and an additional 112 outreach sites. With this number of vaccination sites, the whole population living within 3 km would be covered, and the average traveling distance per person is substantially reduced from 3 km (baseline) to 1.2 km.
anyLogistix is supply chain design software, but, as you’ve seen from this case study, it could easily be applied to other tasks and industries, for example, healthcare-related mass vaccination strategies.
Read the full case study [PDF]: Greenfield Analysis for Vaccination Outreach Strategy.